Search Pattern - CT Head wo
Overview
- Right study open?
- Acute infarct? Voxl 1.
- Bleed? Voxl 2
- Mass effect? Voxl 3
- Ventricles normal? Voxl 3
- Basal cisterns patent? Voxl 3
- Paranasal sinuses clear? Voxl 4
- Bones and mastoid air cells ok? Voxl 4
- Orbital contents ok? Voxl 5
- Scalp and other soft tissue ok? Voxl 5
- Other views ok? Coronal check, focused on bony orbits and pterygoid plates (Voxel 4). Sagittal check, focused on midline brain structures (Voxel 3), clivus and teeth (Voxel 4), nasopharynx and neck (Voxel 5).
0. Do you have the right study open?
- Current study - check the study date, patient name, DOB, and MR# of the study you have open. Are you looking at the study you're supposed to be reviewing? What series are available to you?
- Prior study - pull up the most recent prior study and report. make a note of findings from the prior report. Look for changes between the current and prior study.
- Search pattern - use the normal template to remind you of the search pattern listed here.
1. Is there an acute infarct?
How to look:
W/L: 40/40 Voxl shortcut key: 1, soft tissue axial
This will accentuate grey-white differentiation.
Essential Series:
1. axial reconstruction - brain/soft tissue
Where to look:
Scroll from the vertex (top) through the cerebellum (bottom):
1. cerebral cortex: frontal, temporal, and parietal lobes, insula
2. basal ganglia: caudate, putamen, globus pallidus
3. brainstem: midbrain, pons, medulla
4. cerebellum: cerebellar hemispheres, vermis
What to look for:
1. cerebral cortex: loss of grey-white differentiation.
2. basal ganglia: focal hypodensities.
3. brainstem: focal hypodensities.
4. cerebellum: wedge-shaped hypodensities, easier on sag or coronal.
Key Tips
1. Negative CT Head does not mean there was no stroke. Expect the CT to be negative within first 2 hours from onset, and tiny infarcts may be invisible.
2. Differentiating acute vs chronic stroke is critical.
acute = swelling or no volume loss.
chronic = unchanged relative to prior study, volume loss, adjacent ex-vacuo dilatation of lateral ventricle
2. Is there acute intracranial bleed?
How to look:
W/L: 180/80 Voxl 2, soft tissue axial
This will accentuate blood, including thin epidural and subdural bleeds that hug the inner table of the skull, or trace intraventricular blood in the occipital horns.
Essential Series:
1. axial view - brain/soft tissue
2. coronal view
Where to look: work from outside in
1. Epidural: underneath a skull fracture
2. Subdural: along the left/right convexity, layering along the falx and tentorium
3. Subarachnoid: cerebral sulci, Sylvian fissures, basal cisterns
4. Intraventricular: occipital horns, lateral ventricles, 3rd ventricle, 4th ventricle
5. Intraparenchymal: search everywhere, and focus based on etiology:
• trauma - frontal and anterior temporal contusions, contra-coup (opposite to point of impact), immediate region of impact
• hypertensive - basal ganglia
• amyloid angiopathy - cortical
• mets - cerebral grey-white junction, cerebellum
• vascular malformation - anywhere
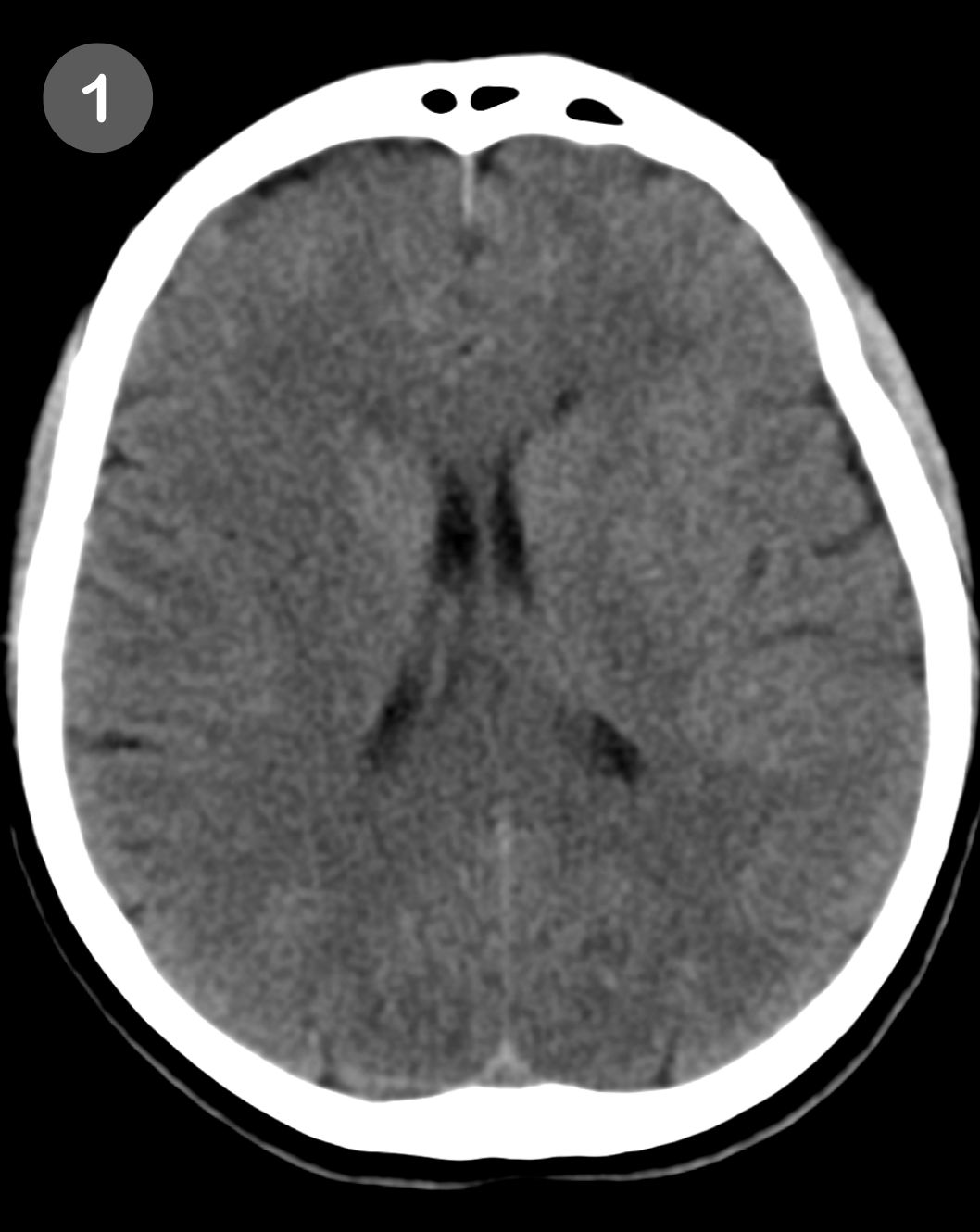


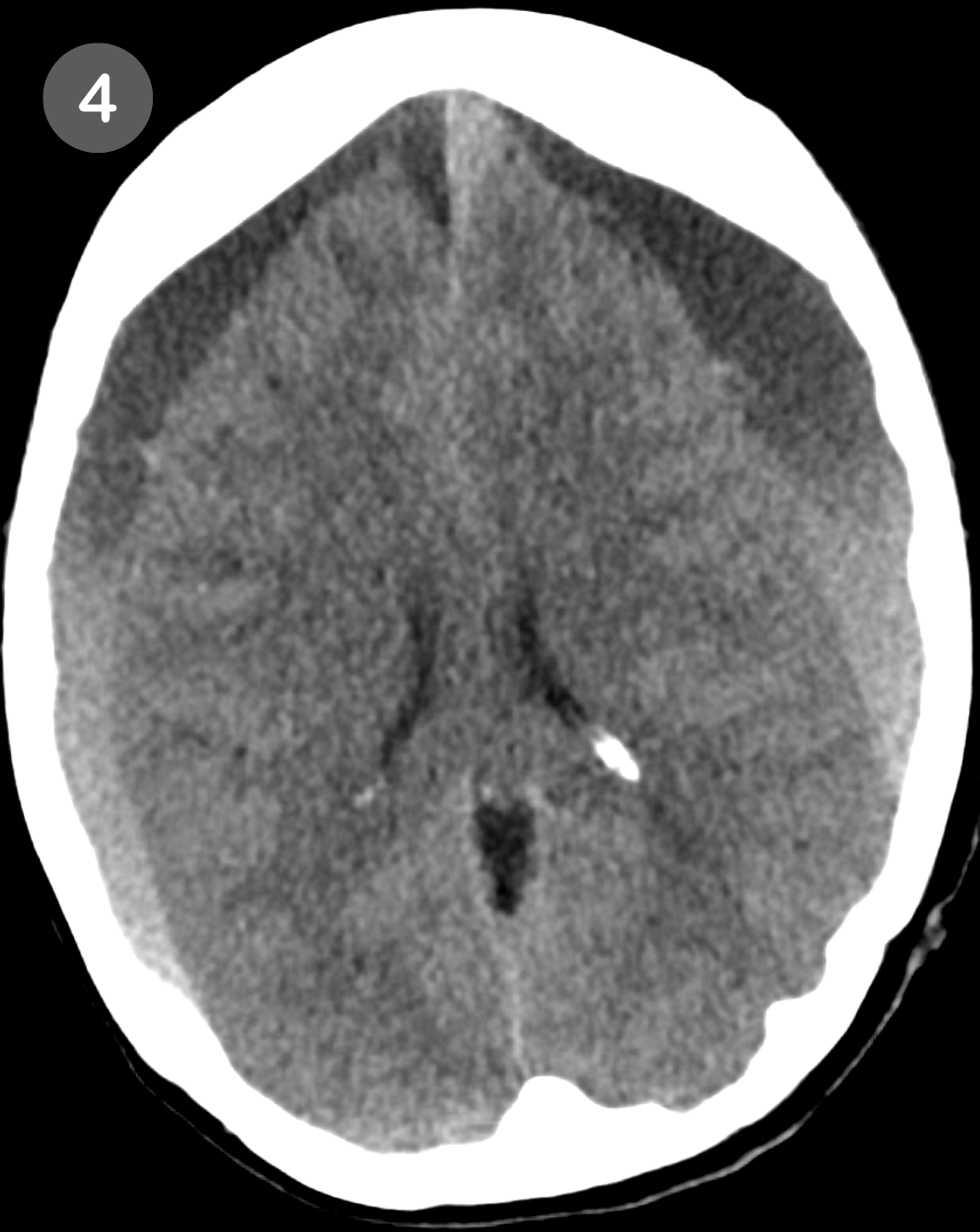
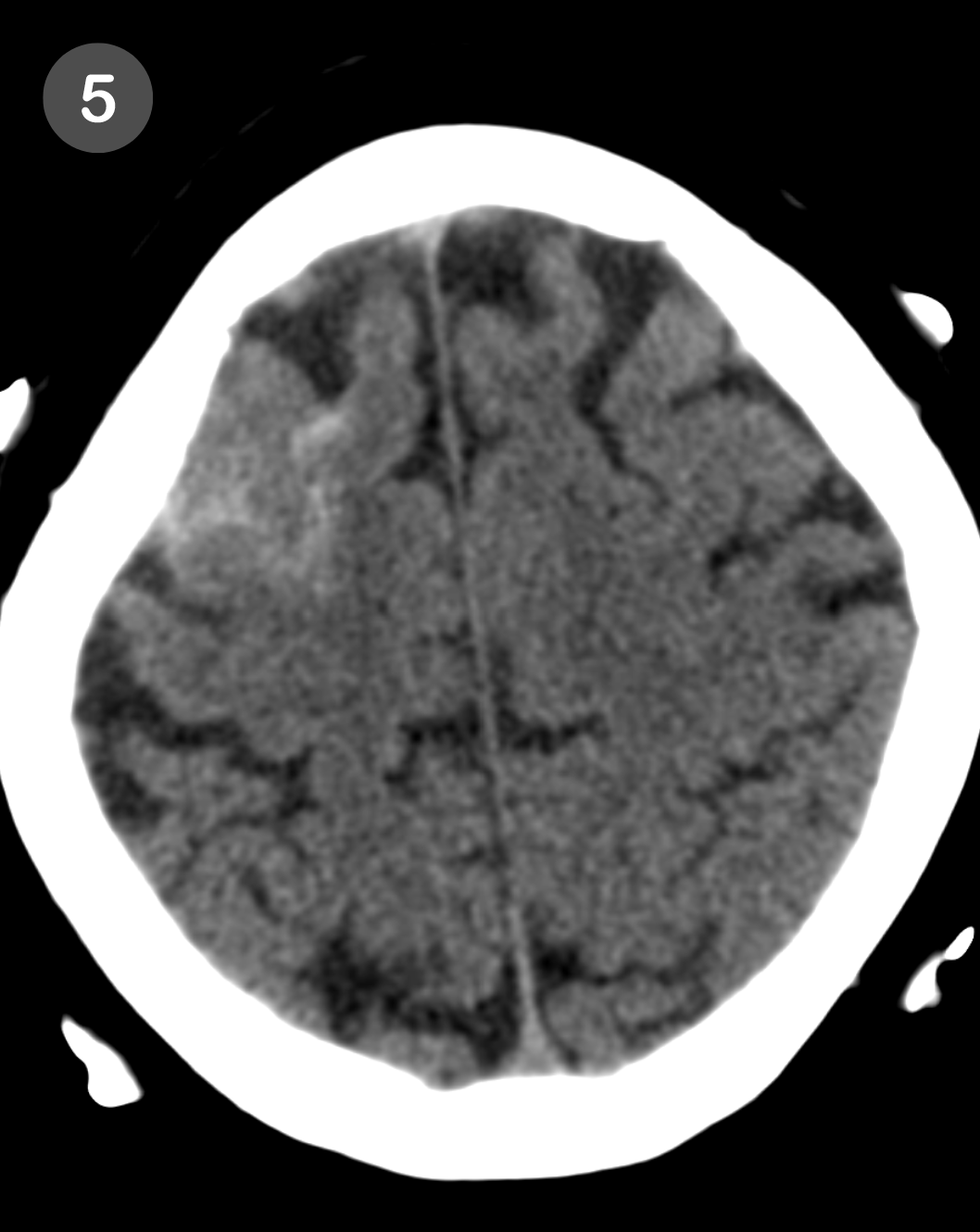

Different types of acute intracranial hemorrhage. (1) Normal, (2) epidural hemorrhage, (3) non-traumatic subarachnoid hemorrhage, (4) subdural hemorrhage, (5) traumatic subarachnoid hemorrhage, (6) intraventricular hemorrhage.
3. Is there mass effect?
How to look:
W/L: 80/40 Voxl 3, soft tissue axial
This will accentuate the brain parenchyma.
Example cases
17 year-old girl unresponsive after MDMA ingestion at electronic music festival. CT shows symmetrical swelling without loss of grey-white differentiation.
64 year-old man unresponsive after cardiac resuscitation. CT shows symmetrical swelling with loss of grey white differentiation. Hypoxic-ischemic injury.
(a) Adequate space at the vertex?
(b) Is the intraventricular septum midline?
(c) Is there adequate space in the sulci at the vertex?
(d) Is there sulcal narrowing locally?
(e) Are the ventricles and basal cisterns narrowed? (steps 3 and 4 for detail)
4. Are the ventricles normal?
How to look:
W/L: 80/40 Voxl 3, soft tissue axial
Ask these questions:
- Are the ventricles small, normal, or enlarged?
- Are the ventricles changed from prior study?
- Is there a mass obstructing the flow of CSF?
- Is the enlargement proportionate to extent of volume loss?
- Is the enlargement asymmetrical between left and right lateral ventricles?
Use these phrases:
Ventricles enlarged out of proportion to extent of volume loss. Differential considerations include normal pressure hydrocephalus, versus central pattern of volume loss.if you see more ventricular enlargement than brain volume loss
Narrowing of the (left/right) lateral ventricle secondary to mass effect, with enlargement of the contralateral ventricle, likely entrapment.if mass effect narrows the lateral ventricle on one side, and the other side is enlarged
Obstructive hydrocephalus.if ventricles enlarged, caused by mass obstructing CSF flow
Examples of obstructive hydrocephalus:
- Colloid Cyst in the Third Ventricle: A colloid cyst located in the third ventricle can obstruct the foramen of Monro, leading to symmetric or asymmetric enlargement of the frontal horns of the lateral ventricles.
- Pineal Tumor or Germinoma: A tumor in the pineal region, such as a pineal germinoma, can obstruct the cerebral aqueduct, causing enlargement of the third and lateral ventricles.
- Cerebellar Tumor: A tumor in the cerebellum can obstruct the fourth ventricle, causing enlargement of the third and lateral ventricles.
5. Are the basal cisterns patent?
How to look:
W/L: 80/40 Voxl 3, soft tissue axial
Look for these patterns of mass effect:
(A) Narrowing of the quadrigeminal plate cistern
(B) Narrowing of the ambient cisterns - as the temporal lobe gets pushed medially
(C) Narrowing of the foramen magnum - represents cerebellar tonsillar herniation, where mass effect pushes the cerebellum downwards, cramming into the foramen magnum. on axial, cerebellar tonsils press into the foramen magnum. on sagittal, inferior tip of the cerebellar tonsils measure > 5mm craniocaudal dimension (CC) from the inner table of the occipital bone.
6. Are the paranasal sinuses clear?
How to look:
W/L: 4000/700 Voxl 4, bone axial
Look for these patterns:
(A) Mucous retention cyst versus polyp
(B) Mucosal thickening - severity (mild, moderate, severe), distributon (circumferential)
(C) Polypoid convexity
(C) Air fluid levels - if high density, mention "likely blood product"
(D) Bony changes - circumferential hyperostosis, erosions, widening of the maxillary sinus antrum, fractures
7. Are bones intact and mastoid air cells clear?
How to look:
W/L: 4000/700 Voxl 4, bone axial
8. Are the orbital contents normal?
How to look:
W/L: 400/40 Voxl 5, soft tissue axial
9. Are the scalp and soft tissues normal?
How to look:
W/L: 400/40 Voxl 5, soft tissue axial
10. Other views ok?
Sagittal check
midline structures (Voxel 3)
clivus (Voxel 4)
nasopharynx
neck (Voxel 5)
Coronal check
Orbits (Voxel 4)
Orbital soft tissue contents (Voxel 5)